Loading...
istanbul_care_clinicFOLLOW US


#1 In Turkey
Istanbul Care is a globally renowned hair transplant brand based in Turkey, and with 3 branches worldwide is known for delivering high-quality procedures at competitive and affordable prices. Through its network of international operation offices, the company ensures convenient access and personalized support for clients from around the world.












We are a medical travel company located in Istanbul, Turkey, operating within the health tourism industry. Under the Istanbul Care brand, we provide high-quality services including hair transplantation, plastic surgery, and weight loss treatments. All procedures are carried out by experienced contracted surgeons in internationally accredited hospitals that are carefully chosen and continuously monitored. Patients from all over the world and from various ethnic backgrounds trust ISTANBUL CARE for safe, professional, and personalized aesthetic healthcare solutions.


Plastic surgery in Turkey has become a preferred choice for patients seeking high-quality aesthetic procedures with natural and long-lasting results. A wide range of treatments is available, performed by experienced surgeons in internationally accredited hospitals that meet strict medical standards. Each procedure is carefully planned according to individual goals, ensuring both safety and patient satisfaction. With advanced techniques, modern facilities, and personalized care, Turkey continues to welcome patients from around the world for trusted and professional cosmetic surgery solutions.

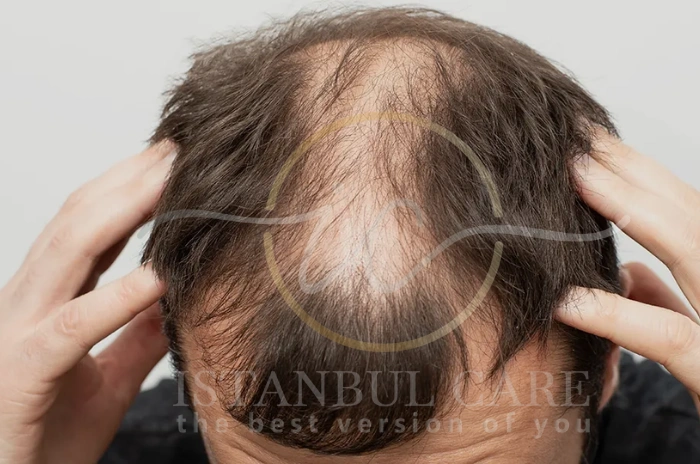
Istanbul is the #1 destination for hair transplantation, renowned for its high success rates, experienced surgeons, and cost-effective treatments. At Istanbul Care, we make the process seamless, ensuring the best results and a hassle-free experience.
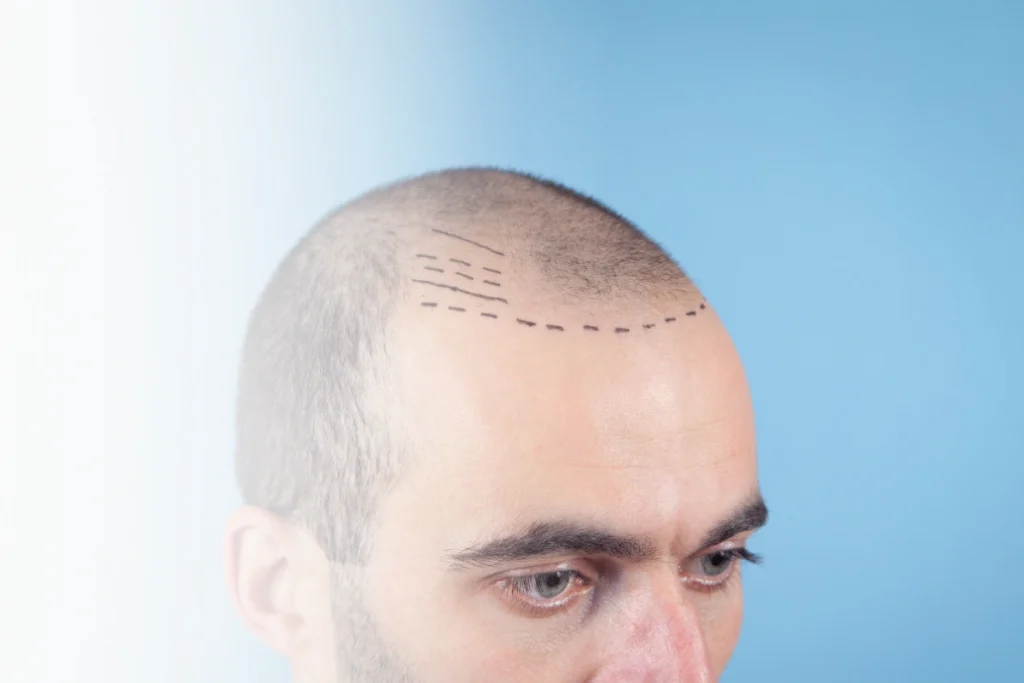
Contact us today and take the first step toward a fuller, thicker head of hair!

Speak with our expert DHI Hair Transplant specialist We're ready to answer your questions

3 weeks ago
I highly recommend Istanbul Care clinic! My husband chose them for a hair transplant and the entire experience was very positive from start to finish. The staff is professional, attentive, and well-trained, and the communication was excellent throughout the whole process. The clinic is modern and clean, and the procedure went smoothly. We are very happy with the results and with the care provided. Thank you, Istanbul Care, for your professionalism and dedication!

a month ago
I loved the overall experience, just wished everybody could speak English better! Also my donor area was not that good so fingers crossed for the results to show. Thanks to the whole team for their support. Turkey has been amazing!

3 months ago
airport to the post-operative evaluation. The hotel was very comfortable and met my expectations. The scheduled pick-up times at the hotel were met. The hospital facilities were also satisfactory. In short, so far I've had a great experience and I recommend it. Now it's just a matter of waiting for the results in the coming months.

3 months ago
Very good throughout the whole process from speaking with the coordinator Tina at the very beginning. The transfered, hotel is lovely and most of all the staff. Treat with dignity and respect throughout highly recomend.

7 months ago
Outstanding Experience – Highly Recommended I had my hair transplant with the support of Claire, and the entire process was genuinely outstanding. From start to finish, she guided me through every step with care, clarity, and professionalism — making what could have been a stressful experience feel completely smooth and reassuring. The clinic staff were equally fantastic: friendly, attentive, and clearly experienced. I felt well looked after from the moment I walked in, and the service throughout was first-class. The results so far have exceeded my expectations, and I’m really happy with how things are progressing. If you’re considering a hair transplant, I can’t recommend this clinic enough. Great team, great care, and great results!
0.0
Average Rating
Over
0
Total Reviews
Over
0
Years of Experience
For those seeking the most successful and natural-looking results, Istanbul Care stands as your number one choice. With over 25 years of expertise, our globally recognized team delivers exceptional hair transplant outcomes that combine advanced medical technology with an artistic touch. Every procedure is customized to your unique features — ensuring a seamless, natural appearance that enhances your confidence and reflects who you truly are. From consultation to recovery, we provide a personalized, world-class experience that thousands of patients from around the world trust and recommend.


When it comes to hair transplant cost in Turkey, especially in Istanbul, few options offer the unbeatable combination of affordability, world-class quality, and truly personalized care like Istanbul Care. As the chart clearly shows, while countries like the USA ($8,000–$30,000), Canada ($10,000–$30,000), Australia ($7,000–$15,000), and the UK ($4,500–$10,000) come with significantly higher price tags, Turkey — and particularly Istanbul — stands out as the most cost-effective destination without compromising on excellence. At Istanbul Care, we provide premium hair transplant procedures (including advanced FUE, DHI, and Sapphire FUE techniques) starting from just $1,990 to $2,490 — often even lower than general averages in Turkey and dramatically more accessible than anywhere else on the list..
Join thousands of satisfied patients who have chosen Istanbul Care for their medical journey. Our state-of-the-art facilities, combined with the expertise of our internationally trained surgeons, ensure the highest standards of care and safety. We offer comprehensive packages that include accommodation, transfers and post-operative care, making your medical journey smooth and stress-free.
























Page 1 of 16